Viagra (Sildenafil) In Testosterne Deficiency Individuals
Testosterone is the most used molecule in male hypogonadism therapy. Other androgenic active ingredients with anabolic action are used for indications (osteoporosis, aplastic anemia, hereditary angioedema, etc.) that do not include the substitution therapy for the androgenic male production deficit. The emphasis on the damage caused by the inappropriate use of these drugs (to increase muscle mass or improve sports performance) has bad light on this therapy by mistakenly extending the use of testosterone to only “substitute” doses the adverse effects of high doses or synthetic products.
Patients with testicular or pituitary damage are by definition the ideal candidate for substitution therapy with testosterone, especially if younger. The use of testosterone at appropriate doses is effective in reestablishing both sex function and androgen-correlated metabolic functions. In these patients, therapy should ideally be conducted for a very long period of time, even beyond reaching adulthood, despite the lack of long and long term safety data. Patients should, however, be advised of the need for regular monitoring of the effects of treatment.
Erectile dysfunction, often improperly indicated by the term “impotence”, is the inability to achieve and maintain a sufficiently high erection to allow a satisfactory sexual intercourse. It is an extremely widespread condition that affects a high percentage male population, which means that millions of Americans have an erection deficit. Although it can occur at any age, erectile dysfunction is more common in men over 45-50 years of age. Aging is therefore one of the major risk factors, also because with aging, different features of erection are modified: increases the time needed to achieve complete rigidity of the penis; it shortens the stage of maintaining the erection, which is also more difficult; it extends refractory period, that is, the time when it is not possible to have another erection after ejaculation.
The mechanism of erection is related to the particular vascularization of the penis and is regulated by the flow of blood in the cavernous bodies (the two dilatable cylinders inside the penis). Under flaccid conditions blood flows into the penis through the arteries and flows, to the same extent, through the veins. In erection this balance is altered by increasing blood flow to the penis and simultaneously reducing venous outflow. It is a sort of electrohydraulic mechanism: following erogenous stimulation (visual, tactile, or even imaginary) some brain areas are activated, which through nerve fibers of the spinal cord stimulate the vascular structures of the penis. The result is a vasodilatation with hyper-affluction of blood to the penis and consequent enlargement and stiffness, which is maintained until ejaculation.
Average age of Canadian Viagra online shopper: is testosterone the key?
Viagra, alongside with other inhibitors of PDE5, is the first-line defence against troubles with sexual function that are caused by severe fluctuations of testosterone levels. Below we will take a closer look at the role of testosterone in a man’s ability of developing and maintaining healthy erections. For now let us just state that the correlation between testosterone levels and erectile function is very close. According to Canadian Health&Care Pharmacy internal statistics, the average age of a Canadian Viagra online shopper is 54.2; 61% of customers ordering Viagra are aged from 50 and above. Further on, we will speak about the connection between ageing, testosterone production and compromised erectile function.
Sildenafil, the active component of Viagra, will be able to help you restore the compromised erectile ability in the absence of the required quantities of the main male hormone; thanks to its mechanism that acts bypassing the hormonal side of the process, Viagra will help you develop steady erections on demand. This, however, does not mean that you should neglect the health issue that has caused the erectile trouble in the first place. You should know that serious deviations from the norm of testosterone production may be harbinger of significant health problems. It is therefore of paramount importance that you seek advice of endocrine health specialist, not just deal with the symptoms of testosterone deficiency.
Viagra integrated in a large-scale testosterone therapy

Hormone therapy involves the intake of testosterone so as to rebalance any deficiency. As has already been pointed out above, testosterone imbalances should not be left unattended. The core reasons for testosterone deficiency should be pinpointed to you by your healthcare provider, be it andrologist, endocrinologist or any other specialist in the field of male hormones, and commeasured actions should be taken in a timely fashion. Viagra or any other ED drug should be used alongside with other products that help maintain testosterone counts within the norm in order to achieve the best therapy outcomes and prevent possible deterioration of your general health condition.
There will be a detailed reference to testosterone deficiency and its consequences at an older age: we will start with pathologies of testosterone production in young. One of its consequences is varicocele, a condition which is traditionally considered an exclusive pathology of fertility affecting the youth population (second – fourth decade). Outside this age range, it seems that the disease hardly exists.
Varicocele is listed among the possible causes of ED in younger individuals and should be treated in order to avoid complications and grave health outcomes; it is therefore not enough to fill your Viagra prescription, although erectile difficulties is the primary concern of many younger patients. Yet varicocele represents a source of continuous and progressive damage to the testis as demonstrated in many studies and it is difficult to imagine that the damage can only be limited to the production of spermatozoa. The testicle as known also has the function of producing testosterone, a task absolved by Leydig cells.
It is only in recent years that importance has been given to testosterone and its decline that is absolutely physiological (normal) over the years, especially after 40-45 years but in some subjects the decline is more pronounced and varicocele may be one of the causes of this decline.
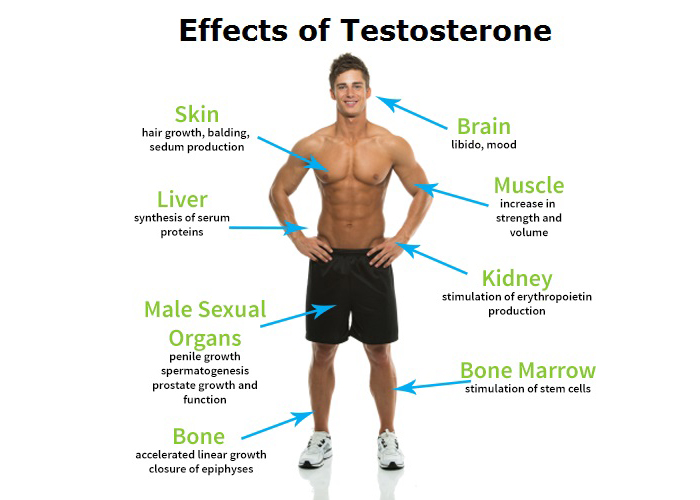
Testosterone is the sex hormone which is par excellence very important for normal sexual function as it improves both indirectly erection and increases libido but testosterone is important for general well-being by acting at various levels in our body: in fact, it improves mood, muscle strength improves muscle strength and muscle mass at bone level facilitates the production of the matrix by making the bones stronger and preventing osteoporosis.
The report is not yet fully verified, but much of the recent studies report a decrease in testosterone in varicocele and often an improvement after varicocele correction. It should also be noted that studies that do not show a direct decrease in testosterone still report the presence of indices of testicular damage to endocrine testicular function (increased LH).
Conceptually, if intervention increases testosterone and testosterone improves the sexual sphere (see above), intervention improves the sexual sphere. It should be noted, however, that there are still few studies in this regard. Among them a personal study also presented at the recent European Sexual Congress held in Milan, out of 82 patients undergoing varicocele correction, 43.9% had a significant improvement in the sexual sphere (at least 4 points of the IIEF score, the questionnaire that measures the quality of the erection).
A diagnosis of hypogonadism should be established before deciding to administer testosterone. Diagnosis should be based on clinical data and should be supported by low serum testosterone levels (total testosterone <2.0-2.4 ng / ml). Moreover, they clearly state the lack of population screening or case-finding screening for other reasons because the mere finding of low testosterone values is not considered sufficient to begin treatment if there are no major clinical problems that can be attributed to the deficit of androgens. Conversely, no treatment should be initiated with normal testosterone levels, despite the presence of suggestive hypogonadic symptoms, as well as ex-adjuvant bipolar therapies should be avoided in patients with a clinical diagnosis but with no hormonal evaluation.
Finally, the guidelines are consistent with the need to establish a proper etiological framing before starting a substitution treatment. Therefore, pathological conditions of male hypogonadism may be excluded, which may also benefit from other treatments (e.g., pituitary lesions to be treated with dopamine agonists or surgery). In some categories of patients most exposed to damage due to defect in antiandrogen production, substitution therapy has been recognized as useful for preventing or treating problems related to testosterone deficiency.
Patients suffering from HIV infection with weight loss and low levels of testosterone have been shown to benefit from a replacement therapy up to 12 months with weight preservation, slowing down the evolution of immunodeficiency indexes, and clinical improvement. Similarly, in patients with severe disease in prolonged treatment with glucocorticoid doses greater than 7.5 mg of prednisone, 6 to 12 months of androgen therapy may improve the symptoms and produce favorable results also on bone mass or on the growth of lean mass.
Testosterone is available in a number of pharmaceutical preparations with different characteristics and modes of use. In recent years, new transdermal, transbuccal and parenteral formulations have been marketed for very long half lives and others will soon be available.
Below we will look at other ways in which testosterone affects erectile function in other age groups.
The role of testosterone in erectile mechanism
Endocrine disorders more closely related to the onset of erectile dysfunction are hypogonadism and hyperprolactinaemia. Hypogonadism results in a reduction in testosterone levels, accompanied by a decrease in sexual desire and a reduction in erectile activity. In men with hyperprolactinaemia, there is an increase in prolactin, which results in an erectile deficit associated with reduced libido and infertility.
In the case of erectile dysfunction, the goal of diagnosis is to define the nature of the disorder: organic, psychological or mixed. The first approach to the diagnostic path consists of an interview (anamnesis) and a IIEF (International Erectile Function Index) questionnaire, specific to focus some aspects of sexual activity (erythema, sexual desire, orgasm stage, degree of satisfaction in sexual intercourse) and lifestyle habits. There follows an objective examination (i.e., the normal direct clinical examination by the physician) and the prescribing of a series of laboratory and instrumental analyses. Laboratory analyses are intended to exclude diabetes or other systemic diseases not previously diagnosed, including glycemia, triglyceridaemia and cholesterolemia, together with the dose of hormones affecting sexual activity (testosterone, dihydrotestosterone, FSH, LH, prolactin and estradiol). Based on the results of this first screening, the doctor will decide whether to continue with second level surveys. These are assessments that allow you to detect venous or arterial changes and monitor nighttime erectile activity. The basal and dynamic penile ecocolordoppler allows to evaluate the correct vascular function of the penis, while night rigidometry (Rigiscan), especially indicated in young patients with erection problems, allows to monitor the nighttime erections that, in the healthy subject, are physiologically present During the REM sleep phase.
Ageing and testosterone levels
Viagra is commonly appointed for use in older citizens. The reasons for that are solid: Viagra has scores of patient-years of proven safety and low side event profile. But did you ever wonder why is that some individuals continue boasting stable and reliable erections well into their 60s and 70s, while others start losing their virility as early as in their fourth decade? If we brush aside other pathologies and pathological self-sabotaging behaviors, when testosterone production comes into play, it is a deciding factor that determines the future development of sexual function of a man.
The inevitable aging phenomenon is accompanied by a progressive decline in testosterone, i.e., serum levels of testosterone. A decline, this, actually rather slow and progressive, which begins inexorably around the age of 25/30 and is inversely correlated with BMI. In other words, the more serious is its overweight status and the greater the chances that the levels of testosterone will drop, even in a relatively early age. The risk, in particular, consists of the sixth decade of life onward.
By examining the results of extensive population studies, starting from 25/30 years of age, the daily testosterone synthesis decreases by 1-2% per year, so that it is almost halved around 70/80 years. In addition to testosterone, the levels of other androgens such as dihydrotestosterone (DHT), DHEA and androstenedione also decreases significantly with age.
In man, testosterone synthesis is entrusted to the testicular cells of Leydig, whose numerical reduction is typically related to the asphalopathy. Not by chance, the testicular volume of an elder is normally reduced compared to that of a young person. Even the hypophyseal center that directs the synthesis of testosterone through the release of LH may prove to be deficient. In particular, the decreased magnitude of the pulsatility of this hormone – in turn controlled by the hypothalamic GnRH (hormone releasing gonadotropins) – is typical of senescence. Let us recall briefly that pulsatility is the phenomenon that a hormone is not secreted steadily over time, but with waves of varying intensity and amplitude, repeated at more or less regular time intervals (the woman’s GnRH pulsateness is strongly related to various stages of the menstrual cycle, while in man it is relatively constant). Precisely for this pulsatility, in the young, serum testosterone levels exhibit a classic circadian pattern (higher in the morning and lower in the evening), which tends to flatten until disappearing in the elder.
To summarize the above, whatever the reasons for testosterone deficiency, it still brings along erectile problems in most cases. Viagra is a safe and effective choice for symptomatic therapy, but close professional monitoring and sometimes testosterone substitution therapy are required in order to both improve the general quality of life and prevent more serious health problems from occurring.





